
{kind=link}
crabsallover highlights, key points, comments / links.
Duane Graveline has a 2012 book 'The Statin Damage Crisis' which got me researching side effects of statins.
Spacedoc aka Duane Graveline says:
'Since the amazing revelation of Ora Shovman on the powerful anti-inflammation action of statin drugs, published in Immunologic Research in 2002 (Abstract and Abstract and Intro), it has been purely a matter of time until an event like the JUPITER trial results of 10 Nov 2008 focused international media attention on this subject.
... Then came statins. With the statins we could lower cholesterol 40 to 50 points. At Johnson Space Center my 270 became 145 in just six weeks with 10 mg of Lipitor. I was overjoyed. Then came my transient global amnesia when for 6 hours I no longer knew my wife or new home. This condition triggered Gravelines' research into statins. Meanwhile hundreds of reports of myopathies, neuropathies and strange neurodegenerative conditions were being reported all associated with the use of statins and none meaningfully reported to the medical community.
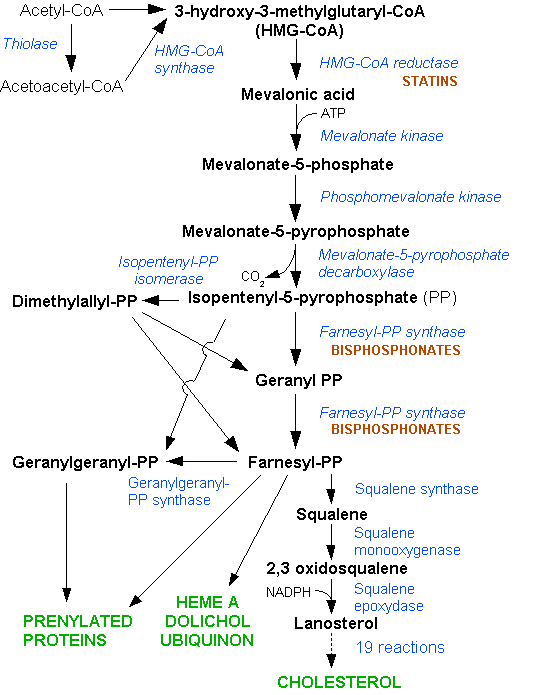
I soon deduced that statin drugs in their officially reported capacity as reductase inhibitors were capable of blockading the critical mevalonate pathway, the biochemical channel for the production of not only cholesterol but Ubiquinone (Coenzyme Q10), dolichols, selenoprotein, Rho?? and altered phosphorylation.
Refs:
Coenzyme q10 and statin-induced mitochondrial dysfunction. Deichmann R, Lavie C, Andrews S. Ochsner J. 2010 Spring;10(1):16-21.
BMJ Case Rep. 2009;2009. pii: bcr07.2008.0412. doi: 10.1136/bcr.07.2008.0412. Epub 2009 Feb 2.
Hepatitis, rhabdomyolysis and multi-organ failure resulting from statin use.
Rajaram M.
Source: St Helens and Knowsley Hospitals NHS Trust, Medicine-Gastro, Whiston Hospital, Warrington Prescot, L35 5DR, UK.
J Am Coll Cardiol. 2007 Jun 12;49(23):2231-7. The role of coenzyme Q10 in statin-associated myopathy: a systematic review. Marcoff L, Thompson PD.
And now it seems that the benefit of statin drugs has been based upon their anti-inflammatory effects alluded to by Shoveman 7 years previously. Astonishingly, it appears cholesterol reduction had nothing to do with it. (Shoveman does not say this) Cholesterol was not our biggest enemy, it was our greatest friend.
We simply cannot not live without ample supplies of cholesterol. It is perhaps the most important biochemical in our bodies, mistakenly turned into a monster by a terribly confused Doctor ?? (who??) now known to have altered his data ?? and a nation ready to welcome a new disease to show what the Federal government could do.
No questions were asked. We only now are learning what the real effects of statins are in our bodies and it is far more that CoQ10 and dolichol inhibition, though that is quite sufficient. Recently we have seen that the primary mechanism of action of statins, the reason so many of the side effects are permanent, is because they are based on mitochondrial mutations.
Adverse Effects of Statins - Mechanisms and Consequences, pp.209-228 (20) Authors: Jerzy Beltowski, Grazyna Wojcicka, Anna Jamroz-Wisniewska - eg Peripheral Neuropathy
With this sad tale behind us we now recognize belatedly that C-reactive protein (CRP) has value as a marker for inflammation. Yes it is a non-specific marker in that an elevated value may just as easily be due to infected teeth, gall bladder or prostate.
This is not a new test. As I recall Ike's CRP was elevated on at least one occasion and in my case it went sky high during a flare-up of diverticulitis 20 years ago that happened to coincide with my astronaut physical as Johnson Space Center. So CRP by itself does not necessarily point to heart disease. Recently it has been refined to help with heart specificity, the hs-CRP (high-sensitivity CRP) test.
C-reactive protein was originally discovered by Tillett and Francis in 1930 as a substance in the serum of patients with acute inflammation that reacted with the C polysaccharide of pneumococcus.
From the very beginning it was known to be associated with a variety of different inflammatory states and as such soon was recognized as a non-specific test for inflammation anywhere in the body.
CRP has no relationship with cholesterol. A person with an elevated CRP can easily be screened for infection in prostate, sinus, teeth, bladder, ovaries or tubes and if found negative becomes suspect for a possible cardiovascular origin and a candidate for use of a low dose statin.
The four elements of inflammation control: platelet activation, monocyte adhesion, lymphyocyte attraction and smooth muscle migration respond very well to the anti-inflammatory impact of any statin, as Shoveman predicted.
Most researchers on this subject believe that certain triggers of inflammation, like homocysteine, cigarette smoking, inherited coagulation defects, inherited platelet defects, transfats, oxycholesterol exposure, etc trigger subendothelial zones of inflammation which if unchecked grow to atheroma.
The use of such markers as the hs-CRP test will allow more judicious selection of candidates for the use of anti-inflammatory drugs. I am confident that both inflammatory markers and anti-inflammatory drugs will drastically improve in time. In the meantime a low dose statin remains an option as do the dietary supplements that are capable of lowering CRP both safely and cost effectively.
Duane Graveline MD MPH
Former USAF Flight Surgeon
Former NASA Astronaut
Retired Family Doctor
Duane Graveline has a 2012 book 'The Statin Damage Crisis' which got me researching side effects of statins.
Spacedoc aka Duane Graveline says:
'Since the amazing revelation of Ora Shovman on the powerful anti-inflammation action of statin drugs, published in Immunologic Research in 2002 (Abstract and Abstract and Intro), it has been purely a matter of time until an event like the JUPITER trial results of 10 Nov 2008 focused international media attention on this subject.
... Then came statins. With the statins we could lower cholesterol 40 to 50 points. At Johnson Space Center my 270 became 145 in just six weeks with 10 mg of Lipitor. I was overjoyed. Then came my transient global amnesia when for 6 hours I no longer knew my wife or new home. This condition triggered Gravelines' research into statins. Meanwhile hundreds of reports of myopathies, neuropathies and strange neurodegenerative conditions were being reported all associated with the use of statins and none meaningfully reported to the medical community.
I soon deduced that statin drugs in their officially reported capacity as reductase inhibitors were capable of blockading the critical mevalonate pathway, the biochemical channel for the production of not only cholesterol but Ubiquinone (Coenzyme Q10), dolichols, selenoprotein, Rho?? and altered phosphorylation.
Refs:
Coenzyme q10 and statin-induced mitochondrial dysfunction. Deichmann R, Lavie C, Andrews S. Ochsner J. 2010 Spring;10(1):16-21.
BMJ Case Rep. 2009;2009. pii: bcr07.2008.0412. doi: 10.1136/bcr.07.2008.0412. Epub 2009 Feb 2.
Hepatitis, rhabdomyolysis and multi-organ failure resulting from statin use.
Rajaram M.
Source: St Helens and Knowsley Hospitals NHS Trust, Medicine-Gastro, Whiston Hospital, Warrington Prescot, L35 5DR, UK.
J Am Coll Cardiol. 2007 Jun 12;49(23):2231-7. The role of coenzyme Q10 in statin-associated myopathy: a systematic review. Marcoff L, Thompson PD.
And now it seems that the benefit of statin drugs has been based upon their anti-inflammatory effects alluded to by Shoveman 7 years previously. Astonishingly, it appears cholesterol reduction had nothing to do with it. (Shoveman does not say this) Cholesterol was not our biggest enemy, it was our greatest friend.
We simply cannot not live without ample supplies of cholesterol. It is perhaps the most important biochemical in our bodies, mistakenly turned into a monster by a terribly confused Doctor ?? (who??) now known to have altered his data ?? and a nation ready to welcome a new disease to show what the Federal government could do.
No questions were asked. We only now are learning what the real effects of statins are in our bodies and it is far more that CoQ10 and dolichol inhibition, though that is quite sufficient. Recently we have seen that the primary mechanism of action of statins, the reason so many of the side effects are permanent, is because they are based on mitochondrial mutations.
Adverse Effects of Statins - Mechanisms and Consequences, pp.209-228 (20) Authors: Jerzy Beltowski, Grazyna Wojcicka, Anna Jamroz-Wisniewska - eg Peripheral Neuropathy
With this sad tale behind us we now recognize belatedly that C-reactive protein (CRP) has value as a marker for inflammation. Yes it is a non-specific marker in that an elevated value may just as easily be due to infected teeth, gall bladder or prostate.
This is not a new test. As I recall Ike's CRP was elevated on at least one occasion and in my case it went sky high during a flare-up of diverticulitis 20 years ago that happened to coincide with my astronaut physical as Johnson Space Center. So CRP by itself does not necessarily point to heart disease. Recently it has been refined to help with heart specificity, the hs-CRP (high-sensitivity CRP) test.
C-reactive protein was originally discovered by Tillett and Francis in 1930 as a substance in the serum of patients with acute inflammation that reacted with the C polysaccharide of pneumococcus.
From the very beginning it was known to be associated with a variety of different inflammatory states and as such soon was recognized as a non-specific test for inflammation anywhere in the body.
CRP has no relationship with cholesterol. A person with an elevated CRP can easily be screened for infection in prostate, sinus, teeth, bladder, ovaries or tubes and if found negative becomes suspect for a possible cardiovascular origin and a candidate for use of a low dose statin.
The four elements of inflammation control: platelet activation, monocyte adhesion, lymphyocyte attraction and smooth muscle migration respond very well to the anti-inflammatory impact of any statin, as Shoveman predicted.
Most researchers on this subject believe that certain triggers of inflammation, like homocysteine, cigarette smoking, inherited coagulation defects, inherited platelet defects, transfats, oxycholesterol exposure, etc trigger subendothelial zones of inflammation which if unchecked grow to atheroma.
The use of such markers as the hs-CRP test will allow more judicious selection of candidates for the use of anti-inflammatory drugs. I am confident that both inflammatory markers and anti-inflammatory drugs will drastically improve in time. In the meantime a low dose statin remains an option as do the dietary supplements that are capable of lowering CRP both safely and cost effectively.
Duane Graveline MD MPH
Former USAF Flight Surgeon
Former NASA Astronaut
Retired Family Doctor
No comments:
Post a Comment